The Difference Between Hazardous And General Medical Waste, Explained
The Difference Between Hazardous And General Medical Waste, Explained
Most healthcare waste is ordinary trash when it’s correctly separated at the source. The key difference: hazardous medical waste is regulated for its chemical properties under RCRA, while general medical waste is non-hazardous, non-infectious material comparable to household garbage. Getting this distinction right protects staff and patients, prevents fines, and lowers treatment costs. A logistics-first program—clear definitions, color-coding, right-sized containers, and verified routing—keeps hazardous streams tight and general streams clean so you don’t overpay for red-bag or RCRA handling. Recycler Routing Guide operationalizes this approach with verified routing and container right‑sizing across every route.
Quick answer to what’s the difference
Hazardous medical waste: Wastes that are listed or exhibit hazardous characteristics—ignitable, corrosive, reactive, or toxic—under RCRA; require a hazardous waste ID, manifests, licensed transport, and specialized treatment/disposal. Common codes include D001–D003 and listed wastes (F/K/P/U) per EPA guidance on RCRA hazardous waste characteristics (EPA waste codes). See the EPA’s technical overview in this EPA guidance on RCRA hazardous waste characteristics (D/F/K/P/U codes): https://iwaste.epa.gov/rpts/EPA_med_haz_watse.pdf
General medical waste: Non-hazardous, non-infectious materials like paper, food, packaging, and clean PPE when properly segregated; typically routed with municipal solid waste. The WHO estimates about 85% of healthcare waste is general, with 15% hazardous or infectious, in its WHO health‑care waste fact sheet: https://www.who.int/news-room/fact-sheets/detail/health-care-waste
Rule of thumb: Most waste is general (~85%). Hazardous or infectious can range 15–35% depending on practice, case mix, and definitions. Misclassification inflates regulated volumes, cost, and compliance risk.
Why the distinction matters for safety, compliance, and cost
Correct segregation cuts exposure risk and keeps regulated volumes small. WHO notes roughly 85% of healthcare waste is general, while up to 0.5 kg hazardous/infectious waste per bed per day can occur in high‑income settings. In the U.S., healthcare produces about 5–6 million tons annually, with an estimated 85–90% being ordinary waste, according to this Reworld Waste guide to compliant medical waste management: https://www.reworldwaste.com/news-and-resources/blog/a-brief-guide-to-compliant-medical-waste-management
Even a 5% swing toward hazardous designation can push tens of thousands of extra tons into costly treatment streams, materially raising contract spend and tip fees. Liability is significant: generators are cradle‑to‑grave responsible, and mishandling has led to large settlements—training programs cite a $49 million case—see Stanford Health Care hazardous waste training: https://stanfordhealthcare.org/content/dam/SHC/health-care-professionals/medical-staff/annual-physician-education/medicalhazardouswasteawarenesstraining25.pdf
Core definitions and regulatory framings
RCRA hazardous waste: A waste is hazardous if it is listed (F, K, P, U) or exhibits a characteristic—ignitability (D001), corrosivity (D002), reactivity (D003), or toxicity (per TCLP). Certain pharmaceuticals are P/U‑listed. Generators, treatment, storage, and disposal facilities (TSDFs) are regulated under RCRA.
Regulated medical waste (RMW)/infectious waste: Clinical materials that pose an infection risk (e.g., sharps, red‑bag waste, pathology). RMW requires infection‑control handling and treatment but is not necessarily RCRA‑hazardous.
OSHA Hazard Communication Standard: Requires labeling and Safety Data Sheets (SDS) for hazardous chemicals; SDS should be accessible at point‑of‑use.
Policy context: Some legacy EPA materials predate the 2019 Hazardous Waste Pharmaceuticals Rule; align procedures with current state and federal updates. See Recycling Today coverage of EPA medical waste guidance: https://www.recyclingtoday.com/news/epa-medical-waste-hazardous-guide-disposal/ Recycler Routing Guide aligns routing and procedures to current federal and state updates, including the 2019 pharmaceuticals rule.
Key criteria that separate the streams
A simple three-step decision flow at the bin:
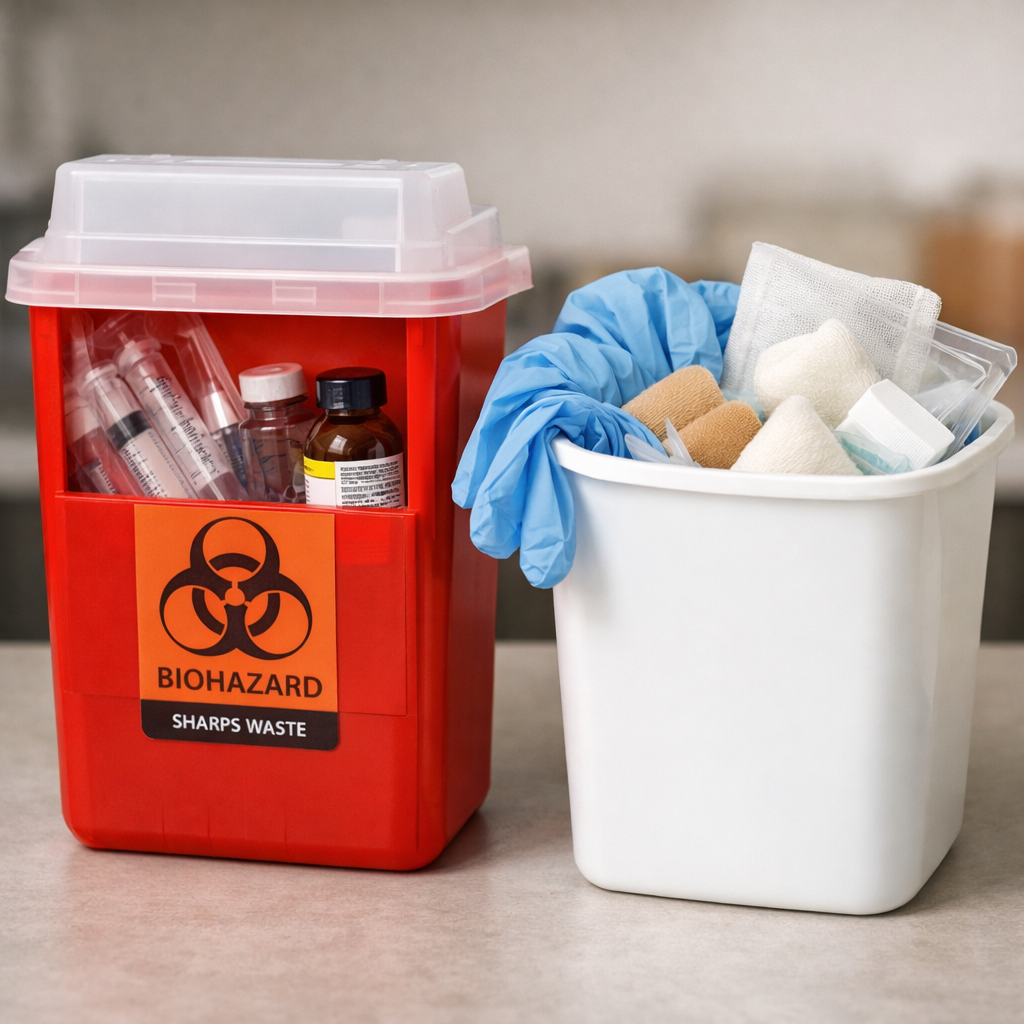
- Is it infectious, visibly contaminated with blood/body fluids, or a sharp? Place in RMW (red bag or sharps), unless it’s also chemically hazardous.
- Does it meet RCRA characteristics or listings (e.g., D001 ignitable solvent, P/U‑listed drugs)? If yes, route as hazardous with a manifest.
- If neither applies, route to general waste. When properly segregated, about 85% fits here.
Mini-definitions of RCRA characteristics:
Ignitable (D001): Liquids with a flash point under 60 °C (140 °F), non-liquids that readily cause fire, or oxidizers that sustain combustion. Examples include alcohol-based solvents, ether, and certain aerosol cans. These require closed, fire-safe storage and compatible containers with grounding when applicable.
Corrosive (D002): Aqueous wastes with pH ≤2 or ≥12.5, or that corrode steel at a specified rate. Typical examples include strong acids/bases used in labs or cleaning (e.g., hydrochloric acid, sodium hydroxide). Segregate acids and bases, use secondary containment, and avoid incompatible co-storage.
Reactive (D003): Unstable under normal conditions, water‑reactive, capable of violent change, releasing toxic gases, or detonating under initiating conditions. Examples include some cyanide/sulfide‑bearing wastes and picric acid crystals. Reactive wastes demand specialized handling; do not mix with water or incompatible materials.
Toxic (TCLP): Contains contaminants above regulatory limits when tested (e.g., mercury, lead, chloroform). Toxicity drives strict handling and treatment to prevent leachate contamination. Keep closed, labeled containers; avoid mixing with non-hazardous materials to preserve proper classification and treatment paths.
Compact decision table:
| Question at bin | Infection risk present? | Chemical hazard present? | Required container/route |
|---|---|---|---|
| Blood/body-fluid contamination or sharps? | Yes | No | RMW: red bag or approved sharps container |
| P/U‑listed or D001–D003/TCLP? | No | Yes | RCRA hazardous container; manifest and permitted transporter |
| Neither | No | No | General waste (clear/black liners); recycle if applicable |
Hazardous medical waste
Scope and examples:
- Pharmaceuticals: P/U‑listed drugs and cytotoxics/chemotherapy agents; expired or partially used meds may be hazardous.
- Chemicals/solvents/reagents: Alcohols, xylene, formalin; ignitable (D001), corrosive (D002), reactive (D003), and TCLP‑toxic wastes.
- Mercury‑bearing items: Broken thermometers, manometers, certain lamps.
Requirements include an RCRA generator ID, proper waste determinations, hazardous waste manifests, and use of permitted transporters and TSDFs, with cradle‑to‑grave responsibility and recordkeeping per EPA Managing Your Hazardous Waste (2019): https://www.epa.gov/sites/default/files/2019-10/documents/10008_managingyourhazwaste_508pdf_october_16_2019.pdf
Apply OSHA labeling, pictograms, and keep SDS available at storage and point‑of‑use stations. Recycler Routing Guide standardizes manifest management and transporter coordination to maintain cradle‑to‑grave compliance.
General medical waste
General medical waste includes materials comparable to household trash: office paper, packaging, cafeteria waste, clean PPE without visible blood, and empty uncontaminated containers. When properly segregated, 85–90% of U.S. healthcare waste is ordinary—keeping it out of red bags avoids unnecessary processing costs and emissions. Use clear or black liners and clear “non‑infectious” labels to reduce confusion, and audit weekly for misplaced red‑bag items. Recycler Routing Guide signage and audits help keep general streams clean.
Regulated infectious waste and sharps
Regulated medical waste covers clinical materials with infection risk (red‑bag waste, sharps, and pathology). It’s governed by OSHA and state/local health departments and is typically treated by autoclave; incineration is reserved for materials that can’t be effectively disinfected. Industry analyses indicate most infectious waste is autoclaved, with a minority incinerated; see the Medical Waste Management Market analysis: https://www.strategicmarketresearch.com/market-report/medical-waste-management-market
Examples:
- Sharps: Needles, blades, broken glass vials/pipettes that can puncture or cut and may be contaminated.
- Pathology: Organs, placentas, and contaminated tissues.
Crossover rule: If sharps or red‑bag items are contaminated with hazardous chemicals (e.g., chemotherapy), they must meet both infection‑control and RCRA requirements. Recycler Routing Guide emphasizes compliant provider selection and documented treatment methods.
Side-by-side comparison of handling and treatment
| Stream | Typical items | Primary regulation | Typical treatment/disposal |
|---|---|---|---|
| Hazardous (RCRA) | P/U‑listed pharmaceuticals; mercury devices; D001–D003 chemicals; TCLP‑toxic wastes | RCRA; manifests; permitted TSDFs | Stabilization/neutralization where applicable; high‑temperature incineration or other RCRA‑compliant treatment as required |
| RMW/Infectious | Red‑bag waste, sharps, pathology | OSHA; state/local RMW rules | Autoclave; incinerate if required by waste type or regulation |
| General (non‑hazardous) | Office paper, packaging, food waste, clean PPE | Municipal solid waste rules | Landfill or recycling where uncontaminated |
| Environmental caution | Open burning/low‑temp incineration | Air‑quality and public‑health risks | Avoid practices linked to dioxins/PM; select compliant, monitored treatment providers |
Cost and routing implications for facilities
Sensitivity: If total healthcare waste is roughly 5.9 million tons, 15% equates to about 885,000 tons designated as infectious/hazardous—small percentage shifts meaningfully change budgets and hauling frequency, per industry market research. Right-size routing to match generation by department:
- Align container counts and sizes by stream; set firm 2–4 hour pickup windows to prevent overflow.
- Use flat-rate quotes with defined weight caps; set caps to departmental baselines to avoid overages.
- Maintain a shared 12‑month reporting window and validate invoices with weighbridge/scale data for audits.
Sample KPIs: hazardous lbs/bed/day vs WHO benchmarks; red‑bag contamination rate; manifest accuracy rate; missed‑pickup rate; overage fee incidence. Recycler Routing Guide supports these controls with shared 12‑month reporting and weighbridge validation.
Recycler Routing Guide
We take a logistics‑first, KPI‑driven approach: confirmed pickup and delivery windows, right‑sized containers, and itemized, flat‑rate dumpster pricing with clear weight caps to prevent surprises. Our verified weighbridge data supports audits and apples‑to‑apples provider comparisons across a shared 12‑month window. Hospitals routinely cut 10–30% by tightening baselines, pulling contract levers, and reinforcing compliance‑focused segregation—we align container mix, manifests, and training cadence to curb hazardous‑designation creep, reduce missed pickups, and improve medical waste compliance across every route.
Logistics-first segregation and container right-sizing
Department‑specific container maps:
- Patient care: Red‑bag and sharps at point‑of‑use; small, sealed pharmaceutical containers in medication rooms; limited general‑waste receptacles to discourage mixing.
- Admin/cafeteria: General waste and recycling prioritized; no red‑bag containers unless clinical functions occur.
Container sizing and liners:
- Use smaller red‑bag containers to limit overuse; larger general‑waste bins with clear/black liners.
- Locking, leak‑proof chem/pharma containers labeled per OSHA Hazard Communication; keep SDS access at stations.
Schedule and routing:
- Weekday sweeps for RMW; hazardous pickups on manifest‑ready days.
- Municipal waste on predictable, load‑factor‑optimized routes with 2–4 hour windows.
Vendor selection, chain of custody, and auditing
Selection checklist:
- Confirm RCRA permits, transporter licenses, OSHA training, and up‑to‑date hazardous medical waste procedures aligned to current pharmaceuticals rules.
- Validate chain‑of‑custody and manifest processes; know your TSDF destinations; keep complete, accurate records.
Audit program:
- Quarterly manifest‑to‑invoice reconciliation; verify weights against scale tickets.
- Random container‑content audits to measure red‑bag contamination and hazardous misclassifications.
Risk reminder: Generators remain cradle‑to‑grave responsible; carefully vet transporters, TSDFs, and recyclers. Recycler Routing Guide documents chain‑of‑custody and TSDF destinations to support audit readiness.
Training, signage, and point-of-use controls
Training plan:
- Role‑based onboarding with annual refreshers; incorporate post‑2019 pharmaceutical rule updates and assign clear responsibilities.
- OSHA Hazard Communication: container labels, pictograms, and SDS access. See the MCF Environmental guide to hazardous medical waste disposal: https://mcfenvironmental.com/hazardous-medical-waste-disposal-a-step-by-step-guide/
Signage and color‑coding:
- Photo‑rich bin signage; red liners for infectious, manufacturer‑labeled yellow/purple for chemo/pharma where required, clear/black for general.
Point‑of‑use controls:
- Sealed sharps containers at eye level within arm’s reach; segregate pharmaceutical waste at med dispensing; ensure general‑waste bins are available to prevent red‑bag overuse.
Common mistakes and how to prevent them
- Red‑bag creep: Clean PPE/packaging tossed into RMW. Fix: smaller red‑bag bins, staff refreshers, and reminders that ~85% is general.
- Mixing chemo or P‑listed drugs into RMW: These are RCRA‑hazardous. Fix: dedicated, labeled containers and controlled access; maintain current P/U lists.
- Inadequate documentation: Leads to fines/liability. Fix: manifest audits, scale‑data validation, and robust chain‑of‑custody logs; remember cradle‑to‑grave responsibility.
Environmental caution: Avoid open burning/low‑temperature incineration tied to dioxins/PM; choose compliant, monitored autoclave/incineration partners.
Surge planning: During outbreaks, medical waste can spike sharply—Wuhan peaked at ~247 tons/day (~6× normal). Build flex capacity and contingency pickups; see an analysis of Wuhan’s medical waste surge: https://pdfs.semanticscholar.org/74e5/2c820795ae40c5581a9fd1cd039d28e51887.pdf Recycler Routing Guide uses scale data and route controls to flag anomalies early and add capacity.
Frequently asked questions
What counts as general medical waste versus hazardous in practice?
General medical waste includes non‑infectious items like office paper, food scraps, and clean PPE, routed like regular trash when segregated. Hazardous medical waste includes listed or characteristic chemicals and certain pharmaceuticals that require RCRA handling and manifests; Recycler Routing Guide applies these criteria in routing maps and training.
Are sharps hazardous, infectious, or both?
Sharps are typically regulated infectious waste due to injury and infection risk and must go in approved sharps containers. If contaminated with hazardous chemicals like chemotherapy agents, they must also meet RCRA hazardous requirements; Recycler Routing Guide provides routing and labeling guidance for both cases.
How should pharmaceuticals be sorted and routed?
Non‑hazardous medications may follow non‑RCRA pharmaceutical programs, but P/U‑listed or cytotoxic drugs are hazardous and require labeled containers, manifests, and permitted transport to specialized facilities. Recycler Routing Guide templates and container maps help keep these streams separate and compliant.
What treatment methods apply to each waste type?
Infectious waste is commonly autoclaved, with incineration used when required; hazardous chemical and pharmaceutical wastes follow RCRA‑compliant treatment or incineration. General waste goes to municipal landfill or recycling when uncontaminated; Recycler Routing Guide documents providers and methods for audit readiness.
How can facilities verify invoices and avoid overage fees?
Match manifests and scale tickets to invoices, track weights by stream, and set flat‑rate contracts with defined weight caps. Recycler Routing Guide supports this with weighbridge validation, firm pickup windows, and right‑sized containers to prevent overages.